Bunions in Newcastle — A Podiatrist’s Guide to What’s Actually Happening (and How Orthotics Help)

That bony lump on the inside of your foot near the big toe joint — you’ve probably been aware of it for years. Maybe it started as a slight prominence you barely noticed. Now it’s red after a long day, your shoes are rubbing it, and you’ve started gravitating toward wider footwear you never used to buy. Perhaps your mother had one. Or your grandmother.
There’s a reason bunions tend to run in families — and it’s not, as many people assume, because they all wore the same bad shoes. Bunions are largely an inherited condition, driven by the underlying mechanics of your foot rather than anything you did wrong. The shoes matter, but they’re accelerants, not causes.
At East Coast Podiatry Clinic in Kahibah, bunions are one of the most common conditions we assess and manage — particularly in women over 40, though we see them across all ages and increasingly in men. This guide covers what a bunion actually is, why genetics are the primary driver, what happens inside the joint as it progresses, and — the part most people don’t know — how custom orthotics can measurably change the forces acting on the joint to slow or stop the progression.
📞 Book an appointment: (02) 4942 2550 · Book online
What is a bunion?
A bunion — the medical term is hallux valgus — is a progressive deformity of the first metatarsophalangeal joint (first MTPJ): the large joint at the base of the big toe.
Despite looking like a growth or a bone that has been knocked out of place, a bunion isn’t either of those things. What you’re seeing is the head of the first metatarsal bone drifting outward (away from the midline of the body), while the big toe angles inward toward the second toe. The “bump” is the metatarsal head becoming more prominent on the inner edge of the foot as it shifts position.
As the deformity progresses, several things happen simultaneously:
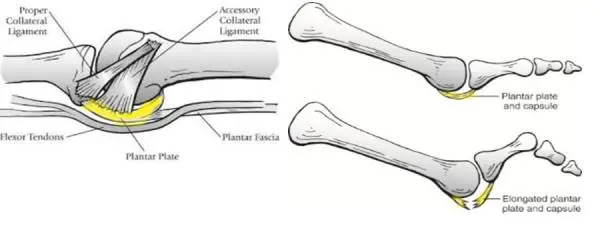
- The joint capsule and surrounding soft tissue stretch and remodel
- The intrinsic muscles of the foot — particularly the abductor hallucis — lose their mechanical advantage and can no longer hold the toe in alignment
- The sesamoid bones beneath the first MTPJ migrate laterally, further destabilising the joint
- The first metatarsal bears less of the body’s weight than it should, transferring load to the second and third metatarsals — which is why bunions are frequently associated with metatarsalgia (ball-of-foot pain), second toe problems, and forefoot callus
Left unmanaged, the big toe can eventually crowd or overlap the second toe. The joint surfaces themselves may undergo arthritic changes. By that stage, surgical correction is often the only remaining option.
Are bunions hereditary?
In most cases, yes — substantially. The research is fairly consistent on this point. Studies suggest that genetic factors account for a significant proportion of bunion risk, with heritability estimates ranging from around 50% to over 80% in some twin studies. If one of your parents has a bunion, your lifetime risk is considerably higher than the general population.
What’s inherited isn’t the bunion itself, but the underlying foot type and joint mechanics that make someone predisposed to developing one:
Hypermobility of the first ray The most important mechanical factor. The first ray (the first metatarsal and the medial cuneiform it articulates with) needs to be stable enough to push off from during gait. In people with inherited hypermobility at this joint, the first ray moves excessively — it dorsiflexes and everts under load rather than staying planted. This causes the forefoot to splay, the first metatarsal to drift medially, and the toe to follow. Hypermobility of the first ray is strongly heritable.
Flat foot (pronated foot type) Overpronation — where the arch collapses and the foot rolls inward excessively during gait — is also largely genetic. It places increased valgus stress on the first MTPJ and contributes to first ray instability. Many patients with bunions also have flat feet, and the two conditions share significant genetic overlap.
Ligamentous laxity Generalised joint hypermobility (loose ligaments throughout the body) is heritable and makes the first MTPJ less capable of resisting the deforming forces of gait.
Metatarsal shape and length The shape of the first metatarsal head and the relative length of the first versus second metatarsal are also inherited traits that influence bunion risk.
So when a patient tells us their mother and grandmother both had bunions, that’s not coincidence — it’s biology. The predisposition is in the structure of the foot, not in the footwear choices.
What footwear actually does Narrow, pointed, or high-heeled shoes don’t cause bunions in feet that aren’t predisposed to them. What they do is accelerate the timeline in feet that are. This is why bunions are more common in women — not because women’s feet are built differently, but because the footwear styles historically worn by women create more compressive and deforming force at the forefoot. Men in narrow dress shoes or steel-capped boots are not immune.
How a bunion actually progresses
Understanding bunion progression requires thinking about the first MTPJ as a joint under load — one that, in a normal gait cycle, bears substantial force hundreds of thousands of times a year.
The normal first MTPJ in gait During normal walking, the heel strikes the ground, the foot rolls forward (pronates slightly), and then resupinates as the foot prepares to push off. At push-off, the first MTPJ dorsiflexes (bends upward) as the body’s weight transfers over the great toe. A well-functioning first MTPJ bears approximately 40–60% of the forefoot’s load at push-off — it is the primary engine of forward propulsion.
For the joint to function properly, the first metatarsal needs to be stable and the toe needs to point straight ahead, so the push-off force travels straight through the joint axis.
What changes with hallux valgus When the first metatarsal begins to drift outward and the toe angles inward, the joint axis rotates. Push-off forces that should travel straight through the joint now act at an angle — creating a moment force that progressively pushes the metatarsal head further outward. The deformity becomes self-reinforcing: the worse the alignment, the more the forces of gait worsen the alignment.
The intrinsic muscles of the foot — particularly the flexor hallucis brevis and abductor hallucis — that would normally act to stabilise and correct this drift are now pulling at the wrong angle. Instead of holding the toe straight, they contribute to the valgus force. The joint is now mechanically compromised from both outside (ground reaction force) and inside (muscle pull).
At the same time, the first metatarsal head — now more prominent and no longer loaded centrally — becomes a pressure point against footwear. The overlying bursa (a fluid-filled sac that forms as a protective response) becomes inflamed. This is the redness and swelling that makes a bunion painful on a bad day.
How orthotics change the forces acting on a bunion
This is the part of bunion management that makes the biggest difference, and the part that’s most poorly understood.
The common misconception is that orthotics “hold the toe in place” or “straighten the joint.” They don’t — and neither does any splint or brace worn during the day. By the time a bunion is visible, the joint has remodelled sufficiently that passive repositioning doesn’t change the structure. What orthotics can do is something more mechanically meaningful: they change the forces acting on the joint during every single step.
Controlling first ray hypermobility The most important mechanical intervention for bunions is stabilising the first ray. A custom orthotic with a specific feature called a first ray cut-out (or first ray relief) allows the first metatarsal head to plantarflex (press downward) under load rather than drifting medially. By supporting the medial arch and preventing excessive pronation, the orthotic keeps the first ray in a more functional position throughout the gait cycle. This reduces the degree to which the first metatarsal splays outward during push-off.
Reducing valgus moment force at the first MTPJ When the foot overpronates, the subtalar joint (just below the ankle) rolls inward, which causes a chain reaction up through the midfoot. The first ray becomes hypermobile, the forefoot splays, and the valgus stress at the first MTPJ increases. A custom orthotic that controls subtalar pronation — through a medial heel post and appropriate arch fill — interrupts this chain at the bottom. Less pronation means less valgus moment force reaching the first MTPJ.
Redistributing forefoot load Metatarsal dome padding or a metatarsal bar built into the orthotic can redistribute load away from the first MTPJ and across a broader area of the forefoot. For patients with concurrent metatarsalgia or pressure callus under the second or third metatarsals, this additional modification significantly reduces discomfort.
Improving push-off mechanics By restoring more normal arch position and first ray stability, a well-designed orthotic allows the first MTPJ to dorsiflexe more efficiently at push-off. Instead of the joint being bypassed (with load transferring to the lesser metatarsals), it can participate more normally in the gait cycle. This reduces the secondary loading on the second and third metatarsals that causes associated forefoot pain.
What the evidence shows The research supports orthotic intervention for bunions most strongly at the mild-to-moderate stage, where the deformity is still progressing and joint congruence is maintained. Studies consistently show that custom orthotics can reduce pain, improve function, and — importantly — slow radiographic progression of the deformity compared to no intervention. They are not a cure, and they do not reverse established deformity. But in a condition where the alternative is progressive joint damage leading to surgery, slowing or halting progression is a clinically meaningful outcome.
The role of footwear alongside orthotics An orthotic can only do so much inside a shoe that is itself creating deforming force. For orthotics to have maximum effect, footwear needs to have adequate toe box width — enough for the toes to sit without lateral compression — and sufficient heel counter stability. A well-fitted custom orthotic in a supportive wide-fit shoe is significantly more effective than the same orthotic in a narrow fashion shoe.
Grading bunion severity
Bunions are typically graded on the severity of the angular deformity, measured on weight-bearing X-ray:
Mild (hallux abductus angle <20°, intermetatarsal angle <11°) The toe has begun to angle but the joint remains largely congruent. This is the stage where conservative management — orthotics, footwear modification, and monitoring — is most effective at slowing progression. Many mild bunions remain comfortable for years with appropriate management.
Moderate (hallux abductus angle 20–40°, intermetatarsal angle 11–16°) The toe angulation is more pronounced, the joint is beginning to sublux (partially dislocate), and the sesamoid bones have begun to migrate. Symptoms are more consistent. Orthotics remain useful for pain management and load redistribution; their ability to slow structural progression diminishes as joint incongruence increases.
Severe (hallux abductus angle >40°, intermetatarsal angle >16°) Significant joint subluxation or dislocation, often with secondary arthritic change. The big toe may crowd or overlap the second toe. Conservative management at this stage is primarily symptom management rather than progression control. Surgical correction may be the only way to restore meaningful function.
When should you see a podiatrist?
The most important thing to understand is that bunions progress — they don’t improve on their own, and they don’t stay stable forever without management. The earlier you’re assessed, the more options you have.
You should book an appointment if:
- You’ve noticed a prominence at the base of your big toe, even if it’s not yet painful
- You have a family history of bunions and want a baseline assessment
- The bunion is causing pain during walking, sport, or by the end of the day
- You’re struggling to find comfortable footwear
- The big toe is beginning to drift toward the second toe
- You’re experiencing associated forefoot pain or callus under the ball of the foot
- You’re considering surgery and want to understand conservative options first
A weight-bearing X-ray (which we can arrange) gives us precise angular measurements to grade the deformity and monitor progression over time. It also tells us whether arthritic change is present in the joint, which influences the management approach.
You don’t need a GP referral to see us — you can book directly.
How we manage bunions at East Coast Podiatry Clinic
There’s no conservative treatment that reverses a bunion. What we can do is manage pain, slow progression, and delay or avoid the need for surgery — which, depending on the severity and your activity level, is often the most practical outcome.
Biomechanical assessment Every bunion consultation starts with a full gait analysis and biomechanical assessment. We look at subtalar motion, first ray mobility, arch position under load, and the way forces are distributed across the forefoot during walking. This tells us exactly what’s driving the deformity in your foot — not all bunions have the same mechanical driver — and guides the orthotic prescription.
Custom orthotics For most patients, a custom 3D-printed orthotic is the central treatment tool. We use precise measurements from a physical assessment to design an orthotic that addresses your specific mechanical pattern — the degree of first ray control, the heel post angle, whether metatarsal modifications are needed. Off-the-shelf insoles don’t provide the same degree of first ray control as a custom device; for a condition where the specific mechanical behaviour of the first ray is the core issue, precision matters.
Footwear advice We assess your current footwear and give specific guidance on toe box width, heel height, and upper construction. This isn’t about aesthetics — it’s about ensuring the mechanical work the orthotic is doing isn’t being undone by the shoe around it.
Padding and offloading For acutely painful or inflamed bunions, gel or silicone bunion shields can reduce pressure from footwear against the joint. Toe separators can reduce lateral pressure from the second toe on the bunion. These are symptom management tools rather than corrective ones, but they significantly improve day-to-day comfort.
Monitoring and X-ray For patients with mild-to-moderate bunions who are managing well conservatively, periodic monitoring — including repeat weight-bearing X-ray every one to two years — allows us to track whether the deformity is progressing or stable. This gives both of us an objective basis for decisions about escalating care.
Surgical referral When conservative management is no longer providing adequate symptom control, or when the deformity has progressed to a point where function is significantly compromised, we refer to an orthopaedic foot surgeon. We can advise on what to expect from different surgical procedures — the most common for moderate bunions is an osteotomy (bone cut and realignment) of the first metatarsal — and what the recovery timeline looks like.
Can I prevent a bunion if it runs in my family?
You can’t change your genetics, but you can change the environment those genetics are operating in. If you have a family history of bunions and you’ve noticed your foot type is similar — flat arch, flexible first ray, tendency to pronate — there’s good reason to be proactive:
- Choose footwear with wide toe boxes and good arch support from early adulthood
- Avoid prolonged wear of high heels or narrow-pointed shoes
- Get a podiatry assessment in your 20s or 30s if you’re concerned, rather than waiting for pain to develop
- Consider a custom orthotic as a preventive measure if your gait assessment shows significant first ray hypermobility or overpronation
- Strengthen the intrinsic foot muscles — foot doming exercises, toe spreads, and short foot exercises all help maintain the dynamic stability that reduces first ray loading
None of this guarantees a bunion won’t develop. But it can significantly extend the period before — if ever — it becomes symptomatic or requires intervention.
Bunion treatment in Newcastle
If you’ve got a bunion that’s getting more noticeable, more painful, or more limiting — don’t wait for it to become a surgical problem. The earlier we assess it, the more we can do.
📍 East Coast Podiatry Clinic, 2/1 Glebe St, Kahibah · 📞 (02) 4942 2550 · 🩺 Book online
Frequently asked questions
Are bunions always painful? Not necessarily, especially in the early stages. Some people have moderate-to-large bunions with relatively little pain; others have small bunions that are acutely painful. Pain level depends on footwear, activity, the degree of associated bursitis, and whether the joint is developing arthritic change. We assess and treat both symptomatic and asymptomatic bunions — the latter because progression is easier to slow before pain develops.
Do bunion splints or toe spacers work? Splints and toe spacers worn at night or during rest can provide temporary symptom relief and may marginally improve toe alignment in mild cases. The research on their ability to slow structural progression is limited. They’re most useful as a comfort aid rather than a corrective device. During activity, when the forces are greatest, a splint can’t compete with ground reaction force — an orthotic worn inside a shoe is far more mechanically relevant.
Will surgery fix it permanently? Modern bunion surgery has good long-term outcomes, particularly minimally invasive approaches. However, because the underlying foot mechanics that caused the bunion don’t change with surgery, recurrence is possible — particularly if footwear habits and biomechanical factors aren’t addressed post-operatively. We recommend continuing orthotic use after surgical recovery for exactly this reason.
How long do orthotics take to work? Most patients notice a reduction in forefoot discomfort within four to eight weeks of consistent orthotic use. Structural changes — slowing of radiographic progression — are assessed over months and years rather than weeks. Orthotics for bunions are a long-term management tool, not a short-term fix.
Can children get bunions? Yes, though less commonly than adults. Juvenile hallux valgus does occur, particularly in children with significant ligamentous laxity or flat feet. It’s worth having assessed early, as children’s bones and soft tissue are still developing and conservative management can be particularly effective at that stage.
Do I need a referral? No. You can book directly online or by phone. If weight-bearing X-rays are needed we can arrange a referral for those.
Will private health cover orthotics? If your extras cover includes podiatry, custom orthotics attract a rebate — the amount varies by fund and level of cover. We can check your eligibility at the time of booking.
Medically reviewed by Tim Foran, Podiatrist (AHPRA registered). Last updated: June 2026.