
Plantar Plate Tears — Why This Forefoot Injury Is So Often Misdiagnosed (A Newcastle Podiatrist’s Guide)
Got a nagging pain under the ball of your foot — right near the base of the second toe — that just won’t settle? Maybe your toe is starting to drift sideways, or sit slightly higher than it used to? You’ve probably been told it’s a neuroma, capsulitis, or “just metatarsalgia.” But there’s a very good chance what you’re actually dealing with is a plantar plate tear — one of the most commonly missed diagnoses in forefoot pain.
Plantar plate tears are notorious for being misdiagnosed, partly because the symptoms overlap with several other conditions, and partly because the plate itself is a structure most people (and a surprising number of clinicians) have never heard of. The result is patients spending months in the wrong treatment — neuroma injections, generic orthotics, even surgery — when the real problem was sitting millimetres away the whole time.
At East Coast Podiatry Clinic in Kahibah, we see this pattern week in, week out (I have actually done this injury twice myself). This post explains what the plantar plate is, why tears get missed, and how we approach diagnosis and treatment for patients across Newcastle and Lake Macquarie.
📞 Book a forefoot assessment: (02) 4942 2550 · Book online
What is the plantar plate?
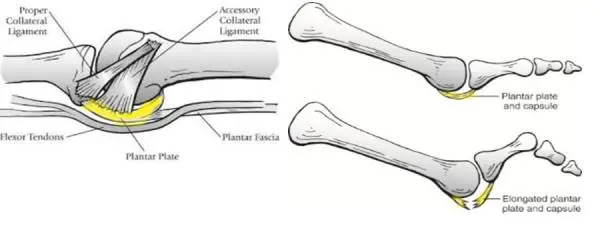
The plantar plate is a thick, fibrocartilaginous ligament that sits on the underside of each metatarsophalangeal joint (MTPJ) — the joints at the base of your toes. Think of it as a small, dense pad of tissue that:
- Supports your body weight as it passes through the ball of the foot
- Holds the toe in alignment with the metatarsal bone
- Stops the toe from hyperextending upwards when you push off
- Stabilises the joint during walking, running, and standing
The plate at the second toe does the most work and takes the most punishment, which is why second MTPJ plantar plate tears are by far the most common. Tears at the third toe happen too, but less often.
When the plate stretches, frays or tears, the joint loses its stabiliser. The toe starts to drift, the joint becomes painful, and over time the toe can deviate, elevate, or even cross over its neighbour.
What does a plantar plate tear feel like?
Classic features include:
- Aching, burning, or bruised-feeling pain under the ball of the foot, usually at the base of the second toe
- A sensation that you’re “walking on a pebble” or that your sock is bunched up
- Swelling on top of or under the affected joint
- The toe lifting slightly off the ground when standing — the “floating toe” sign
- The toe drifting sideways, often towards the big toe (a developing crossover toe)
- Pain on push-off when walking, running, or going up stairs
- A feeling that the toe is unstable or “loose”
- Pain that’s worse barefoot on hard floors and better in supportive shoes
The pain is usually gradual in onset, often starting after a period of increased load — new exercise, more walking, a job that’s harder on the feet. Less commonly, a sudden injury (a stub, a hyperextension) can rupture the plate acutely.
Why is it so often misdiagnosed?
This is the question we get most often, and there are a few reasons.
1. The symptoms overlap with Morton’s neuroma. Both cause forefoot pain, both can produce numbness or burning, both feel worse in tighter shoes. But a neuroma sits between the metatarsal heads (most often between the third and fourth), while a plantar plate tear sits underneath the joint (most often the second). The treatments are completely different. A neuroma injection won’t touch a plantar plate tear — and we see plenty of patients who’ve had two or three injections before anyone questioned the diagnosis.
2. It gets lumped in with “capsulitis” or “metatarsalgia.” Both are real conditions, but they’re often used as catch-all terms when a clinician knows something’s wrong in the ball of the foot but hasn’t pinned down what. A plantar plate tear is a form of capsulitis in the strict sense, but the management is more specific and the prognosis without proper treatment is worse — the deformity progresses.
3. Imaging often misses it. Standard X-rays don’t show soft tissue, so they look “normal.” Ultrasound can pick up plantar plate tears but is highly operator-dependent — and many sonographers don’t routinely scan for it unless specifically asked. MRI is the gold standard but is rarely ordered for forefoot pain in the early stages.
4. The clinical test isn’t well known. The most sensitive bedside test is the modified Lachman’s (drawer) test — gently pushing the base of the toe upwards relative to the metatarsal head to see if there’s excessive movement. It takes about five seconds and tells you a lot, but it’s not part of most general assessments.
5. The early signs are subtle. A toe that’s “just slightly higher” or “drifts a few degrees” doesn’t trigger alarm bells for someone who isn’t specifically looking for it. By the time the toe is visibly crossing over, the tear has usually been there for months or years.
Who gets plantar plate tears?
The risk profile is fairly predictable:
- Women over 40 — particularly common, often associated with years of narrow or high-heeled footwear
- People with a long second toe (Morton’s foot) — the second metatarsal absorbs disproportionate load
- Runners and high-impact athletes — repeated forefoot loading is a major driver
- People with bunions — as the big toe drifts, more load transfers to the second
- People with high arches or stiff first rays — pressure shifts laterally to the second MTPJ
- People with inflammatory arthritis — the plate is weakened from within
A sudden increase in load — a walking holiday, a new running program, switching to minimalist or zero-drop shoes — is a common trigger in an already vulnerable foot.
When should you see a podiatrist?
The earlier the better. Book in if:
- You’ve had ball-of-foot pain for more than 2–3 weeks
- Your second toe is starting to look different — higher, drifting sideways, sitting separately from the others
- You can feel a “pebble in your shoe” that isn’t there
- Forefoot pain has been treated as a neuroma but isn’t improving
- You’ve noticed a gap forming between your second and third toes
- Pain is worse with push-off, barefoot walking, or running
Catching a plantar plate tear at the partial-tear stage is dramatically easier than catching it once the toe has fully dislocated dorsally. Conservative treatment works well in the early stages. Once the toe is visibly crossing over, you’re often looking at surgery.
How we treat plantar plate tears
The first visit is about confirming the diagnosis (clinical tests, often supported by ultrasound or MRI referral), grading the tear, and identifying what drove it — foot shape, footwear, activity load, biomechanics.
First phase — offload and protect
- Taping the toe down into a plantarflexed position — this is the single most important early intervention. It takes load off the plate and prevents further drift.
- Activity modification — reducing high-impact forefoot loading while the plate settles
- Stiff-soled or rocker-soled footwear to limit toe-off bending through the painful joint
- Short-term anti-inflammatories for symptom relief if appropriate
Second phase — support and rehabilitate
- Custom 3D printed orthotics with a metatarsal dome or pad positioned to offload the affected joint specifically — generic met pads often sit in the wrong place and make things worse
- Footwear changes — a stiff forefoot shoe, often with a rocker sole, makes a significant difference
- Targeted toe strengthening — intrinsic foot muscle exercises and toe-flexion work to restore active toe control
- Calf and forefoot mobility work — a tight calf increases forefoot load and slows recovery
For more advanced tears
- Ultrasound or MRI to assess the extent of the tear and rule out other pathology
- Referral to a sports physician or orthopaedic foot and ankle surgeon if the toe is dislocated, crossing over, or not responding to conservative care
- Surgical repair is well established for higher-grade tears — it involves reattaching or reconstructing the plate, and outcomes are good in the right candidates
The goal of conservative care is to stop the progression. We can’t always “heal” the tear itself — fibrocartilage has limited healing capacity — but we can stabilise the joint, prevent further drift, and get you out of pain.
Why early treatment matters so much
Plantar plate tears progress in a predictable way: partial tear → toe elevates → toe drifts medially → crossover toe → dislocation. Each step makes treatment harder and outcomes worse. A patient who walks in at the “floating toe” stage has far more conservative options than one who walks in with a fully crossed-over second toe.
The other reason is that the longer a tear is left, the more secondary problems develop — calluses under the joint, neuroma-like nerve symptoms from the altered loading, bunion progression, hammertoe deformity of the affected toe. Treating the original tear early avoids cascading problems further up the chain.
Preventing recurrence
Once a plantar plate tear has settled, keeping it settled is largely about managing load:
- Wear your orthotics consistently, especially during exercise and long days on your feet
- Stick with stiffer-soled, supportive footwear and avoid prolonged barefoot walking on hard surfaces
- Keep up with toe strengthening — long term, not just until the pain settles
- Be cautious with sudden increases in walking, running, or high-impact activity
- Get any return of “pebble in the shoe” sensation looked at early
- Annual review so we can track any subtle changes in toe position
Book a forefoot assessment in Newcastle
If you’ve got ball-of-foot pain that won’t settle, or you’ve noticed your second toe is sitting a bit differently to the others — get it checked properly. The earlier we look, the more options you have.
📍 East Coast Podiatry Clinic, 2/1 Glebe St, Kahibah · 📞 (02) 4942 2550 · 🩺 Book online
Frequently asked questions
Can a plantar plate tear heal on its own? Small, partial tears can stabilise with proper offloading, taping, orthotics and footwear changes — but the fibrocartilage itself rarely “heals” the way a muscle would. The aim of conservative treatment is to stop the tear progressing and get you out of pain.
Will I need surgery? Most early-stage tears (where the toe is still in reasonable alignment) respond to conservative care. Surgery becomes the main option when the toe has dislocated or is significantly crossing over.
How is it different from a Morton’s neuroma? A neuroma is a thickened nerve sitting between the metatarsals (usually between the third and fourth). A plantar plate tear is damage to the ligament under the joint (usually the second). They feel similar but the treatment is completely different — which is why getting the right diagnosis matters.
How long does conservative treatment take? Expect 3–6 months for meaningful improvement, with ongoing orthotic and footwear support long term to prevent recurrence.
Can I still run with a plantar plate tear? Often yes in the early stages, with the right offloading, footwear and load management. More significant tears usually require a temporary reduction in high-impact activity.
Do I need a referral? No — you can book directly. We can co-manage with your GP, sports physician or orthopaedic specialist if needed.
Medically reviewed by Tim Foran, Podiatrist (AHPRA registered). Last updated: May 2026.


