
That Burning Pain in the Ball of Your Foot? It Could Be Morton’s Neuroma — A Newcastle Podiatrist Explains
Feels like you’re walking on a pebble — or a sock bunched up under your toes — but there’s nothing there? That’s the classic description of a Morton’s neuroma, and it’s one of the more common causes of forefoot pain we see in clinic. The good news is that most cases settle well with conservative treatment, particularly when caught early. The frustrating part is that they rarely go away on their own — and the longer the nerve stays irritated, the harder it is to calm down.
At East Coast Podiatry Clinic in Kahibah, we assess, treat and manage Morton’s neuromas for patients across Newcastle and the Lake Macquarie area.
📞 Book an assessment: (02) 4942 2550 · Book online
What is a Morton’s neuroma?
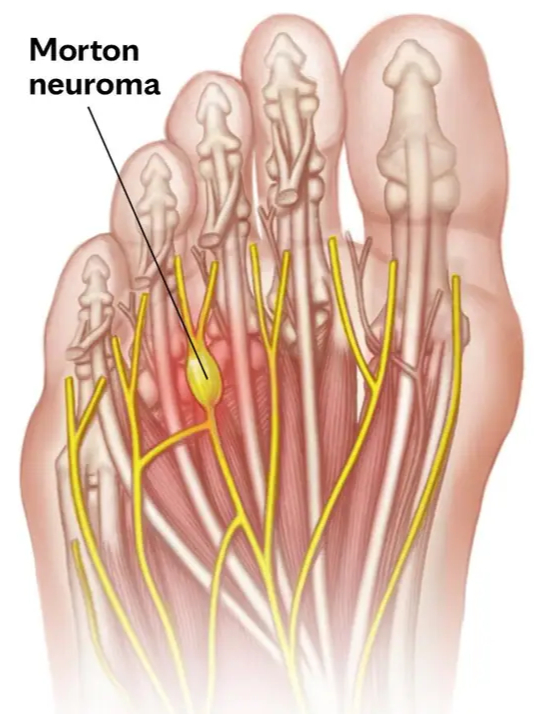
A Morton’s neuroma is a thickening of the tissue around one of the nerves that runs between the bones of your forefoot (the metatarsals). Despite the name, it’s not actually a tumour — it’s a benign nerve irritation caused by chronic compression.
The nerve sits in a tight channel between the metatarsal heads, and when it’s squeezed repeatedly — by narrow shoes, high heels, or biomechanical issues that shift load onto the forefoot — the surrounding tissue thickens. That thickening narrows the channel further, the nerve becomes inflamed, and the symptoms begin.
It most commonly affects the nerve between the third and fourth toes, though the second/third interspace is also a regular offender.
What does it feel like?
Morton’s neuroma has a fairly distinctive pattern. Most people describe at least a few of these:
- A burning, sharp, or shooting pain in the ball of the foot
- The sensation of a pebble, marble, or bunched-up sock under the foot
- Numbness, tingling, or “electric shock” feelings into the third and fourth toes
- Pain that’s dramatically worse in tight or narrow shoes
- Relief when the shoe comes off, often with the urge to massage the foot
- Symptoms that worsen with walking, standing for long periods, or running
Many patients tell us they’ve taken to kicking their shoes off under the desk at work, or stopping mid-walk to slip a heel out and rub the front of their foot. That pattern is classic.
How do Morton’s neuromas happen?
Most Morton’s neuromas we see in clinic come from a combination of:
- Footwear — narrow toe boxes, high heels, stiff dress shoes, and pointed work shoes
- Repetitive forefoot loading — running, walking long distances, sports with lots of pivoting
- Foot shape — bunions, hammertoes, high arches, and flat feet all change forefoot mechanics
- Occupational standing — nurses, hospitality staff, teachers, tradies in stiff work boots
- Tight calves — limited ankle range pushes more load through the forefoot with every step
It’s also significantly more common in women aged 40–60, largely driven by years of narrower footwear.
When should you see a podiatrist?
Not every episode of forefoot pain needs a professional visit, but see someone soon if:
- The pain has been present for more than a couple of weeks
- You feel a click, marble, or shifting sensation when walking
- Numbness or tingling is travelling into the toes
- You’re changing the way you walk to avoid the pain
- Shoes that used to be comfortable now aren’t an option
- Pain is interfering with sport, work, or daily walking
Early assessment helps you avoid the two biggest mistakes people make: persisting in the wrong footwear until the nerve is significantly thickened, or living with it for so long that it stops responding to conservative care.
How we treat Morton’s neuroma
The reassuring news is that the majority of Morton’s neuromas respond well to conservative treatment. Surgery is only required in a small minority of cases. Here’s how the typical treatment plan looks:
First steps — settle the nerve
- Footwear assessment and change — this is the single most important step. Wider toe box, lower heel, stiffer sole through the forefoot
- Metatarsal padding — a small pad placed just behind the metatarsal heads splays the bones apart and offloads the nerve. Often gives noticeable relief at the first visit
- Activity modification for high-impact loading, particularly for runners
- Ice and short-term anti-inflammatory measures for symptom relief
Ongoing — fix the underlying mechanics
- Custom 3D printed orthotics — built specifically for your foot shape and gait pattern, with metatarsal support built directly into the device to offload the nerve long-term
- Calf and intrinsic foot stretching to reduce forefoot loading
- Strengthening of the small foot muscles that support the metatarsal arch
- A footwear plan that works for your work, sport and everyday life
If conservative care isn’t enough
- Referral for ultrasound-guided corticosteroid or alcohol sclerosing injection in stubborn cases — we work closely with local radiologists when this is needed
- Surgical referral for the small number of cases that don’t respond — typically a neurectomy or decompression procedure
If your biomechanics are part of the problem — a foot type that overloads the forefoot, a bunion, or a tight calf — we’ll address that as part of the plan. A neuroma that’s settled but the underlying cause left untouched is a neuroma that tends to come back.
Why early treatment matters
The longer a nerve stays compressed, the more thickened and sensitive it becomes. Early-stage neuromas often settle within 4–8 weeks of starting treatment. Long-standing neuromas that have been ignored for a year or more are more likely to need injection therapy or surgical referral.
The other thing worth knowing: changing one variable usually isn’t enough. Just switching shoes, or just adding a metatarsal pad, or just getting an orthotic in isolation often gives partial relief. The patients who get the best long-term outcomes are the ones who address footwear, padding/orthotics, and the underlying mechanics together.
Preventing a recurrence
If you’ve had a Morton’s neuroma settle, you can cut your risk of it returning by:
- Sticking with wide-toe-box, low-heel footwear as your everyday default
- Reserving narrow or heeled shoes for short occasions, not full days
- Replacing running and walking shoes before they’re packed out (typically every 600–800km)
- Keeping calves and feet mobile with regular stretching
- Continuing to use orthotics or metatarsal padding if they were part of what got you better
Book a forefoot assessment in Newcastle
If you’ve been walking around with that “pebble under the foot” feeling — or kicking your shoes off every chance you get — we can help.
📍 East Coast Podiatry Clinic, 2/1 Glebe St, Kahibah · 📞 (02) 4942 2550 · 🩺 Book online
Frequently asked questions
How long does a Morton’s neuroma take to settle? Early cases often improve within 4–8 weeks of starting treatment. Long-standing or larger neuromas can take 3–6 months, and a small number need injection or surgical input.
Will a Morton’s neuroma go away on its own? Rarely. Without addressing the footwear or mechanics causing the compression, the nerve stays irritated and the tissue keeps thickening. Most cases need some form of intervention.
Do I need an ultrasound or MRI? Not always — most Morton’s neuromas can be diagnosed clinically. Imaging is useful when the diagnosis is unclear, the neuroma is large, or we’re considering an injection.
Are cortisone injections safe for Morton’s neuroma? They can be very effective for stubborn cases, but repeated injections aren’t recommended due to the risk of fat pad atrophy. They’re generally a second-line option after conservative care.
Can I still run with a Morton’s neuroma? Often yes, with the right footwear, metatarsal padding or orthotics, and some short-term load management. Pushing through significant pain tends to make things worse.
Do I need a referral to see a podiatrist? No — you can book directly. We can also liaise with your GP, sports physician or specialist if other care is involved.
Medically reviewed by Tim Foran, Podiatrist (AHPRA registered). Last updated: May 2026.


