
Plantar Fasciitis vs Plantar Fasciosis — What’s the Difference?
If you’ve had heel pain for any length of time, you’ve probably been told you have “plantar fasciitis.” It’s one of the most common diagnoses in podiatry — affecting roughly 1 in 10 people at some point in their life — but the name itself is actually a bit misleading. In many cases, what’s really going on isn’t an inflammation of the plantar fascia at all. It’s a degeneration of it. And the difference matters, because it changes how we treat it and how long it takes to get better.
At East Coast Podiatry Clinic in Kahibah, we treat heel pain for patients across Newcastle and the Lake Macquarie area every week. Here’s what you need to know.
📞 Book a heel pain assessment: (02) 4942 2550 · Book online
What is the plantar fascia?
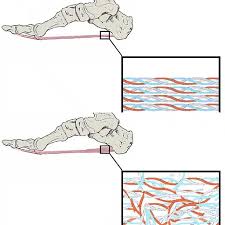
The plantar fascia is a thick, fibrous band of tissue that runs along the bottom of your foot, connecting your heel bone (the calcaneus) to the base of your toes. Think of it as a cross between a tendon and a ligament. Its job is to support the arch and absorb the shock of every step.
Every time you walk, run or stand, the plantar fascia takes load. When the load you put on it exceeds what it can tolerate — over hours, weeks or years — that’s when the trouble starts.
Plantar fasciitis — the “-itis” version
The suffix “-itis” means inflammation. Plantar fasciitis, in the strict sense, refers to an inflammatory process in the plantar fascia — usually caused by a sudden overload or microtearing of the tissue.
Classic plantar fasciitis tends to look like this:
- Sharp heel pain with the first few steps in the morning, easing once you get moving
- Pain that returns after long periods of sitting (the “first step after the couch” pain)
- Tenderness on the inside of the heel where the fascia attaches to the bone
- Onset often linked to a clear trigger — a sudden increase in running, a long day on your feet, new shoes, or a holiday spent walking on hard surfaces
This is the version most people picture when they hear “plantar fasciitis,” and when it’s caught early it usually settles within a few weeks of proper treatment.
Plantar fasciosis — the “-osis” version
The suffix “-osis” refers to a degenerative process — not inflammation, but a breakdown of the tissue itself. Plantar fasciosis describes chronic plantar fascia pain where the underlying problem is no longer inflammation but collagen breakdown, microscarring and thickening of the fascia.
Plantar fasciosis tends to look like this:
- Heel pain that has been hanging around for months, not weeks
- Pain that’s less “sharp inflammation” and more “deep, persistent ache”
- Symptoms that flare up, settle a little, then flare again — the classic chronic pain cycle
- A plantar fascia that often feels thickened or lumpy on examination
- Resistance to standard anti-inflammatory treatments (because there’s no longer much inflammation to treat)
This is what plantar fasciitis can quietly become if it isn’t properly addressed. The repeated microtearing and incomplete healing leads to scar tissue and a fascia that’s structurally weaker and less able to handle load.
Plantar fasciopathy — the umbrella term
To make things slightly more confusing, current best-practice terminology in podiatry and sports medicine now leans toward plantar fasciopathy as the overall name for the condition. The reason is that most people sit somewhere on a spectrum — they have some inflammation and some degeneration at the same time, with one usually being the dominant driver.
So instead of asking “is it fasciitis or fasciosis?”, a better question is often: “Where on the spectrum is this person?”
- A runner with two weeks of sudden heel pain after ramping up training is probably 80% inflammation, 20% degeneration
- A teacher with 18 months of grumbling heel pain that won’t settle is probably 80% degeneration, 20% inflammation
- Plenty of people sit somewhere in the middle
That distinction matters because the treatment for each end of the spectrum is genuinely different.
Why the difference matters
When you treat the wrong end of the spectrum, you waste time — and sometimes make things worse.
For the inflammatory end (fasciitis):
- Relative rest and load reduction help quickly
- Ice and short-term anti-inflammatories can settle symptoms
- Stretching and taping give noticeable relief within days to weeks
- Most cases resolve within 6–12 weeks with proper care
For the degenerative end (fasciosis):
- Rest alone often doesn’t fix it — the tissue needs a stimulus to remodel
- Anti-inflammatories have little effect because there’s not much inflammation left
- Progressive loading exercises (calf raises, heavy-slow resistance work) become central to recovery
- Treatment is measured in months, not weeks — typically 3–6 months for meaningful improvement
- Shockwave therapy, custom orthotics and biomechanical correction become more important
- Injection therapies (PRP in particular) may be considered in stubborn cases
This is why “I rested it for a month and it didn’t help” is such a common story in chronic heel pain. If the underlying problem is degeneration rather than inflammation, rest doesn’t load the tissue enough to stimulate repair.
When should you see a podiatrist?
Not every twinge of heel pain needs a professional visit. But book in if:
- Heel pain has been present for more than 2–3 weeks
- The “first step in the morning” pain is becoming routine
- You’ve already tried stretching, new shoes and over-the-counter inserts without much improvement
- The pain is affecting sport, work, or how much you walk in a day
- You’re starting to change the way you walk to avoid the pain
- You’ve been told you have “plantar fasciitis” before and it keeps coming back
Early assessment helps you avoid the most common mistake we see: persisting with the wrong treatment until acute fasciitis quietly becomes chronic fasciosis. The sooner we know where on the spectrum you are, the more targeted the treatment plan.
How we treat heel pain
At East Coast Podiatry Clinic, we don’t use a one-size-fits-all heel pain protocol. The first visit is about working out where on the fasciitis–fasciosis spectrum you sit, identifying the contributing factors (foot type, calf tightness, training load, footwear, body weight, occupation), and building a plan from there.
First phase — settle symptoms
- Taping (low-dye or arch-supporting strapping) for immediate offloading
- Footwear advice — switching to shoes that actually support the arch
- Calf and plantar fascia stretching program
- Activity modification rather than complete rest
Second phase — rebuild capacity
- Custom 3D printed orthotics designed for your specific foot shape and gait, to offload the fascia long-term
- Progressive loading program — heel raises with appropriate progression to stimulate fascia remodelling
- Strengthening of the small foot muscles and the calf complex
- Gradual return to running, sport or extended standing
Advanced options for stubborn cases
- Shockwave therapy
- Referral for ultrasound assessment to quantify fascia thickness and rule out other diagnoses
- Referral for corticosteroid or PRP injection where appropriate
- Co-management with sports physicians or orthopaedic specialists in the rare cases that need it
If your biomechanics are part of the problem — a flat foot, a high arch, tight calves, or weak hip stabilisers contributing to overloading the fascia — we’ll address that as part of the plan. A fascia that’s settled but the underlying cause left untouched is a fascia that tends to flare up again.
Preventing a recurrence
If you’ve had plantar fasciitis or fasciosis settle, you can reduce your risk of it coming back by:
- Maintaining calf and foot mobility with regular stretching
- Replacing running and walking shoes before they’re packed out (every 600–800km)
- Avoiding rapid increases in training load — the “10% rule” still holds
- Continuing to use orthotics or supportive footwear if they were part of getting you better
- Keeping body weight in a range that doesn’t overload the fascia
- Strengthening the foot and calf complex, even when you’re symptom-free
Book a heel pain assessment in Newcastle
If your heel has been hurting for more than a couple of weeks — or you’ve been chasing the same “plantar fasciitis” diagnosis for months without lasting relief — let’s work out what’s actually going on and get a proper plan in place.
📍 East Coast Podiatry Clinic, 2/1 Glebe St, Kahibah · 📞 (02) 4942 2550 · 🩺 Book online
Frequently asked questions
How do I know if I have fasciitis or fasciosis? As a rule of thumb, pain that’s been around for less than 6 weeks and responds to rest is probably more fasciitis. Pain that’s been around for 3+ months, doesn’t settle with rest, and isn’t responding to anti-inflammatories is more likely fasciosis. A clinical assessment (and sometimes ultrasound) can clarify.
Will plantar fasciitis go away on its own? Sometimes — but research shows that about 80% of cases improve within 12 months with proper treatment. Without it, untreated fasciitis often progresses to fasciosis, which takes much longer to resolve.
Are cortisone injections a good idea? They can help short-term for an inflammatory flare-up, but they don’t address the underlying problem and repeated injections can weaken the fascia. They’re generally a second-line option.
Do I need an ultrasound or MRI? Most cases are diagnosed clinically. Imaging is useful when the diagnosis is unclear, the pain isn’t responding to treatment, or we’re considering injection therapy. Ultrasound can show fascia thickness and rule out partial tears or other diagnoses.
Can I keep running with plantar fasciitis? Often yes — with modified volume, the right footwear and possibly taping or orthotics. Pushing through significant pain tends to extend the recovery. We’ll work out a sensible plan with you.
Do I need a referral to see a podiatrist? No — you can book directly. We can co-manage your care with your GP or other specialists if needed.
Medically reviewed by Tim Foran, Podiatrist (AHPRA registered). Last updated: May 2026.


