Synovitis of the Second MTPJ — A Newcastle Podiatrist’s Guide to Ball-of-Foot Pain
Ever felt a deep, achy pain in the ball of your foot — right at the base of the second toe — that gets worse the longer you’re on your feet? It’s one of the more underdiagnosed causes of forefoot pain we see in clinic, and it has a name most people have never heard: second MTPJ synovitis. The good news is that when it’s caught early, it settles well with conservative treatment. The bad news is that left untreated, it can progress to a more serious problem called plate plantar instability that’s far harder to fix.
At East Coast Podiatry Clinic in Kahibah, we assess and treat synovitis for patients across Newcastle and the Lake Macquarie area.
📞 Book a forefoot assessment: (02) 4942 2550 · Book online
What is synovitis?
Every joint in your body is lined by a thin layer of tissue called the synovium. Its job is to produce synovial fluid — the lubricant that keeps the joint moving smoothly and comfortably. When the synovium gets irritated, it produces too much fluid and becomes inflamed. That’s synovitis.
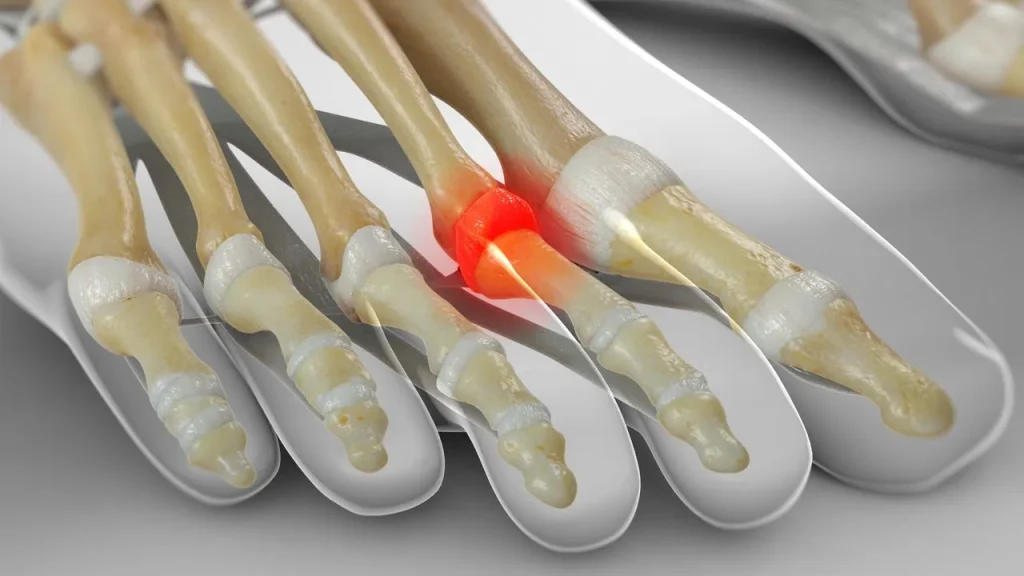
Synovitis can affect any joint, but in the foot we see it most often at the second metatarsophalangeal joint (MTPJ) — the joint where the long bone behind your second toe meets the base of the toe itself. It can also affect the first MTPJ (around the big toe) and the smaller joints further down the toes, but the second MTPJ is by far the most common.
Why the second MTPJ?
The second toe joint takes more load than people realise. When you push off with each step, a huge amount of force travels through the ball of the foot — and the second metatarsal often bears the brunt of it.
A few things make this joint particularly vulnerable:
- The second metatarsal is often the longest bone in the forefoot, which means it strikes the ground harder
- It sits right next to the big toe, so when the big toe isn’t pulling its weight (bunions, hallux limitus, stiffness) the second toe takes over
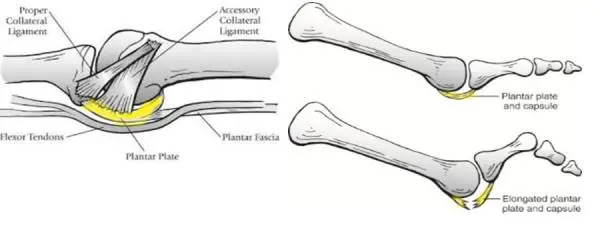
- The joint is held in place by a small structure called the plantar plate, which can stretch or tear under repetitive load
- Anything that increases forefoot pressure — high heels, tight shoes, running, jumping — gets concentrated here
What does it feel like?
The classic presentation of second MTPJ synovitis includes:
- Sharp or aching pain in the ball of the foot, right at the base of the second toe
- Pain that’s worse with weight-bearing — walking, running, standing for long periods
- A feeling that you’re walking on a small lump under the second toe
- Swelling on the top or bottom of the foot near the second toe
- The second toe may start to drift sideways (usually towards the big toe) or lift slightly off the ground
- Pain that improves with rest and worsens again as soon as you’re back on your feet
The “lifted toe” sign is important — it suggests the plantar plate is starting to give way, and that’s the point where the condition becomes much harder to reverse.
How does it happen?
Most cases we see come from a combination of:
- Repetitive overload — running, jumping sports, long days on hard floors, high-mileage walking
- Foot mechanics — bunions (hallux valgus), a long second metatarsal, hammertoes, flat feet, or a stiff big toe joint
- Footwear — high heels concentrate force on the forefoot; narrow toe boxes squeeze the joints
- Inflammatory arthritis — rheumatoid arthritis and other inflammatory conditions can target the MTPJs
- Sudden increase in activity — picking up running after a break, a new fitness program, a long holiday on your feet
It’s also more common in women over 40, particularly those who’ve worn high-heeled or narrow shoes for years.
When should you see a podiatrist?
Not every ache in the ball of the foot needs a professional visit. But book in if:
- The pain has been around for more than 2–3 weeks
- It’s affecting how much you walk, work or exercise
- The second toe is starting to look different — drifting, lifting, or sitting higher than the others
- You can feel a swelling or lump under the joint
- Over-the-counter inserts and rest aren’t fixing it
- You’ve been told you have a “Morton’s neuroma” but treatments for it aren’t working (synovitis is often misdiagnosed as neuroma)
Early treatment is genuinely important here. Synovitis that’s caught in the inflammatory phase usually settles within weeks. Synovitis that’s been left for months can progress to plantar plate tear and toe deformity — and that’s a much bigger problem to manage.
How we treat synovitis
The first visit is about confirming the diagnosis, ruling out other causes of forefoot pain (Morton’s neuroma, stress fracture, capsulitis), and identifying why the joint became overloaded in the first place.
First phase — settle the inflammation
- Taping — strapping the toe in a slightly plantarflexed position offloads the joint immediately and often gives noticeable relief at the first visit
- Metatarsal padding — a small pad placed just behind the joint redistributes pressure
- Activity modification — reducing the impact loading while the joint settles
- Ice and short-term anti-inflammatories for symptom relief
- Footwear review — switching to shoes with a stiffer sole, lower heel and wider toe box
Second phase — fix the underlying mechanics
- Custom 3D printed orthotics built specifically to offload the second MTPJ, with integrated metatarsal support
- Strengthening of the small foot muscles and toe flexors
- Calf stretching to reduce forefoot loading
- A footwear plan that protects the joint long-term
If conservative care isn’t enough
- Referral for ultrasound imaging to assess the plantar plate and rule out a tear
- Corticosteroid injection — used selectively, because repeated steroid injections can weaken the plantar plate
- Surgical referral in the small number of cases that have progressed to plantar plate tear with toe deformity
If a bunion, hammertoe or stiff big toe is the underlying driver, we need to address that too — otherwise the synovitis tends to come back.
Why early treatment matters
The reason we treat synovitis early is that the synovium itself isn’t the only structure at risk. Sitting underneath the joint is the plantar plate — a strong band of ligament that holds the toe in place. Chronic synovitis stretches and weakens this plate, and once it tears, the toe begins to drift or lift. At that point, conservative care can manage symptoms but can’t fully reverse the deformity.
Six weeks of focused treatment in the early stage is far easier than years of managing a deformed toe.
Preventing a recurrence
If you’ve had MTPJ synovitis settle, you can reduce your risk of it coming back by:
- Sticking with wide-toe-box, low-heel footwear as your everyday default
- Continuing to use orthotics or metatarsal padding if they were part of getting you better
- Building forefoot strength with toe flexor and calf exercises
- Replacing running shoes every 600–800km
- Avoiding rapid increases in training load — the “10% rule”
- Treating bunions or stiff big toe joints rather than letting them progress
Book a forefoot assessment in Newcastle
If you’ve got that nagging ache at the base of your second toe — or you’ve noticed the toe starting to look different — let’s get it assessed before it progresses.
📍 East Coast Podiatry Clinic, 2/1 Glebe St, Kahibah · 📞 (02) 4942 2550 · 🩺 Book online
Frequently asked questions
How is synovitis different from a Morton’s neuroma? They both cause ball-of-foot pain but in different places. Synovitis is at the joint at the base of the second toe (often with swelling and toe drift). A neuroma is between the third and fourth toes (with burning, tingling and a “pebble” feeling). Clinical assessment usually distinguishes them.
Will it go away on its own? Sometimes mild cases settle with rest and shoe changes alone. More often it needs targeted treatment — and the longer you leave it, the higher the risk of plantar plate damage.
Do I need an ultrasound or MRI? Most cases are diagnosed clinically. Imaging is useful when we suspect a plantar plate tear, or when symptoms aren’t responding to treatment.
Are cortisone injections safe? They can help in stubborn cases, but we use them carefully because repeated injections can weaken the plantar plate and make a tear more likely.
Can I keep running? Often yes, with reduced volume, the right shoes, and possibly taping or orthotics. Pushing through significant pain tends to make it worse.
Do I need a referral? No — you can book directly. We can co-manage with your GP or sports physician if needed.
Medically reviewed by Tim Foran, Podiatrist (AHPRA registered). Last updated: May 2026.