Hammertoe Treatment in Newcastle
That toe that won’t lie flat anymore? It’s probably hammertoe — and the earlier you act, the more options you have. In its early stages hammertoe is flexible and very treatable without surgery. Once the joint becomes rigid, options narrow. Most people we see in clinic have lived with it for years before booking, often because they assumed it was “just how their feet are now.” It isn’t.
At East Coast Podiatry Clinic in Kahibah, we assess and treat hammertoe and related toe deformities for patients across Newcastle and Lake Macquarie.
📞 Book an assessment: (02) 4942 2550 · Book online
What is hammertoe?
Hammertoe is a deformity where one of the smaller toes bends downward at the middle joint, so the toe looks like an upside-down V. It most commonly affects the second toe but can happen to any of the lesser toes.
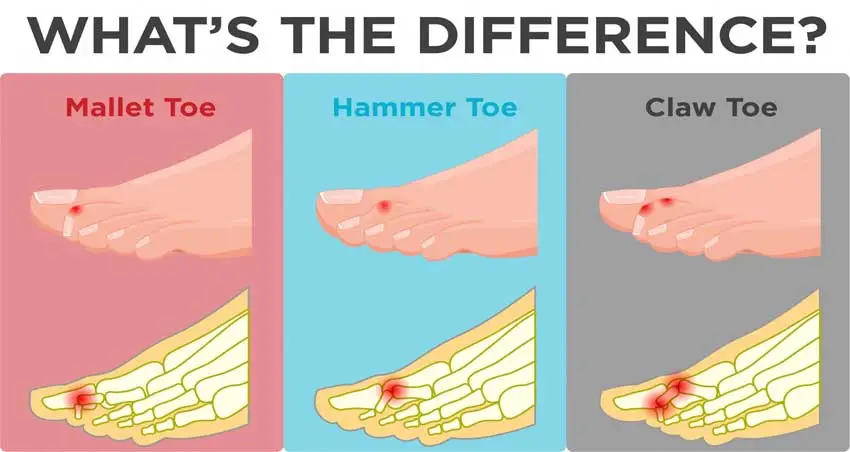
It’s part of a family of toe deformities that often get confused:
- Hammertoe — bend at the middle joint (PIP). The most common.
- Claw toe — bend at both middle and end joints, with the base joint also pulled upward. Usually affects multiple toes at once and is often linked to nerve issues.
- Mallet toe — bend at the end joint (DIP) only. The tip of the toe points downward.
The treatment principles overlap, but the underlying cause and best approach differ — which is why a proper assessment matters before you spend money on splints or pads.
Early signs — and why they matter
In the early stage, the affected toe is still flexible. You can straighten it with your fingers, and it lies flat when you’re barefoot. This is the window where conservative treatment works best.
Over time, the tendons on the underside of the toe shorten and the joint capsule tightens. The toe gradually becomes rigid — stuck in the bent position even when nothing is pushing on it. Once a hammertoe is fully rigid, non-surgical treatment can manage pain and pressure but generally can’t reverse the deformity.
Common symptoms we see:
- A toe that visibly bends or sticks up
- Corns on top of the bent joint where it rubs the shoe
- Calluses under the ball of the foot (the metatarsal head takes more load)
- Pain when wearing shoes, especially anything narrow
- Burning or aching in the forefoot after standing
- Difficulty finding shoes that fit
What causes hammertoe?
Hammertoe is almost always a combination of factors rather than a single cause:
- Footwear — narrow toe boxes and high heels push toes into a bent position and, over years, the soft tissue adapts to that shape. This is the single biggest factor in most cases.
- Foot structure — a long second toe, a bunion pushing the big toe sideways, high or flat arches, or a forefoot that splays under load
- Muscle imbalance — the small muscles inside the foot (intrinsics) weaken with age, while the longer tendons keep pulling. The toes “buckle” as a result.
- Nerve and neuromuscular conditions — diabetes, peripheral neuropathy, Charcot-Marie-Tooth disease and stroke can all change the muscle balance in the foot
- Previous injury — a stubbed or broken toe that healed in a slightly bent position
- Genetics — hammertoe often runs in families, particularly where a long second toe is inherited
It’s more common in women (largely a footwear issue) and increases with age. But it’s not inevitable.
When to see a podiatrist
Earlier is better. The best time to see us is when:
- The toe still bends when you press on it (flexible stage)
- Corns or calluses are starting to form on or around the toe
- Your shoes are getting harder to find or wear
- You have diabetes or any nerve condition — even mild toe deformity needs monitoring because pressure points can ulcerate
- The toe is painful, red, or has broken skin
If the toe is already rigid and pain-free, you may still benefit from an assessment to prevent secondary problems (calluses, metatarsalgia, ulceration if you’re high-risk).
How we treat hammertoe
Most hammertoes can be managed without surgery, particularly when they’re caught early. Here’s how we approach it:
1. Footwear review This is the foundation. Most hammertoes started with shoes, and no other treatment will hold up if you keep wearing the shoes that caused the problem. We’ll go through what you’re currently wearing and suggest changes — usually a wider toe box, a stiffer sole, and a heel under 3 cm.
2. Padding, splinting and offloading Silicone toe sleeves, crest pads and hammertoe splints can take pressure off corns, separate rubbing toes, and gently stretch the flexor tendons in flexible-stage hammertoes. These are simple, cheap, and often dramatically reduce day-to-day pain.
3. Custom orthotics If the underlying issue is biomechanical — and it usually is — orthotics can offload the metatarsal heads, support the arch, and stop the toes being driven into a bent position with each step. Particularly useful when there are calluses under the ball of the foot.
4. Corn and callus management The skin lesions hammertoe causes are themselves painful. We can debride corns and calluses in clinic, which gives immediate relief while the longer-term plan does its work.
5. Toe exercises and stretching For flexible hammertoes, daily toe stretches and intrinsic-muscle strengthening (towel scrunches, toe spreads, marble pick-ups) can slow progression and sometimes partially reverse the deformity. We’ll teach you the ones that suit your foot.
6. Surgical referral — when it’s needed For rigid, painful hammertoes that aren’t responding to conservative care, surgery is an option. We don’t perform foot surgery in clinic but we’ll refer you to a podiatric or orthopaedic foot surgeon and co-manage your pre- and post-operative care. Surgery is usually a day procedure and recovery takes 4–8 weeks.
Living with hammertoe — practical tips
- Buy shoes in the afternoon — feet swell during the day, so a shoe that fits at 4pm will be comfortable all day
- Measure your feet — most adults are wearing shoes a half-size to a full size too small, particularly width
- At least 1 cm of space between your longest toe and the front of the shoe
- Soft, seamless uppers over the bent joint to reduce corn formation
- Avoid skin-on-skin contact between toes — a thin silicone sleeve prevents the corns that form between rubbing toes
- Skip the bathroom razor on corns — file gently with a pumice but don’t cut into them; that’s how infections start
Preventing hammertoe
You can’t change your foot structure or your genetics, but you can change what you put on your feet:
- Wider toe boxes, lower heels, day to day
- Save the dress heels for short stretches, not all-day wear
- Keep the intrinsic muscles strong — barefoot time, toe exercises, balance work
- Address bunions and other foot problems early — they change how load passes through the toes
- If you have diabetes, get a diabetes foot assessment yearly even when nothing hurts
Book a hammertoe assessment in Newcastle
If a toe is starting to bend, rub or hurt — or you’re tired of shopping for shoes that fit — we can help. The earlier we see it, the more we can do.
📍 East Coast Podiatry Clinic, 2/1 Glebe St, Kahibah 📞 (02) 4942 2550 🗓️ Book online
Frequently asked questions
Can hammertoe be fixed without surgery? Yes, in most cases — particularly while the toe is still flexible. Footwear changes, orthotics, splinting and exercises can manage symptoms and slow progression. Once a hammertoe becomes rigid, non-surgical treatment manages pain rather than straightening the toe.
Will hammertoe get worse if I leave it? Usually, yes — slowly. The tendons gradually shorten and the joint stiffens. The deformity that’s flexible today may be rigid in a few years. Conservative treatment is most effective in the early, flexible stage.
Do toe straighteners and splints actually work? For flexible hammertoes, yes — they help. They don’t work for rigid hammertoes (the joint has fused into position). The right type matters; an over-the-counter splint that’s too aggressive can cause more pain than it solves. A podiatrist can recommend or fit the right device.
Why are my second toes the worst? The second toe is often the longest in the foot, so it hits the front of the shoe first and bends to fit. People with a “Morton’s toe” (long second toe) are particularly prone.
Is hammertoe surgery worth it? For rigid, painful hammertoes that aren’t responding to conservative care, surgery has good outcomes — most people are very satisfied. It’s not a quick decision though; recovery is 4–8 weeks and you’ll need to commit to the rehab. We help patients weigh up the timing.
Are hammertoes covered by health insurance? Private health extras usually cover podiatry appointments (depends on your level of cover). Orthotics may be partially covered. Surgery, if needed, is generally a Medicare item with a private health gap. We can talk you through what to expect.
Medically reviewed by Tim Foran, Podiatrist (AHPRA registered). Last updated: May 2026.