Ingrown Toenail Treatment in Newcastle — A Podiatrist’s Guide to Getting Lasting Relief
Got a toenail that’s red, swollen, and agony to touch the moment your sock brushes it? Maybe you’ve been trying to manage it at home — cutting a V in the nail, digging at the corner, stuffing cotton wool under the edge — and finding it settles for a week or two, then comes back worse than before. Or maybe it’s been infected, your GP put you on antibiotics, and the antibiotics helped, but the problem is still there.
Ingrown toenails are one of the most common conditions we see at East Coast Podiatry Clinic in Kahibah — and they’re also one of the most persistently self-treated, often incorrectly, for months before someone comes in to get it properly sorted.
This guide covers what actually causes an ingrown toenail, why the home remedies don’t fix the underlying problem, what treatment looks like, and — importantly — how to prevent it from recurring.
📞 Book an appointment: (02) 4942 2550 · Book online
What is an ingrown toenail?
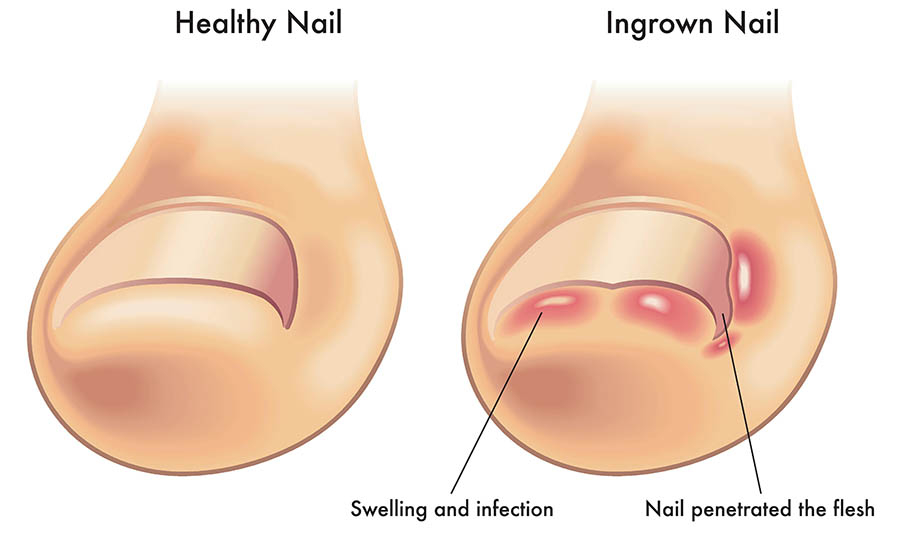
An ingrown toenail — medically known as onychocryptosis — occurs when the edge or corner of the toenail grows into the surrounding skin (the nail sulcus) rather than over it. The result is inflammation, pain, and, if left long enough, infection.
The big toe is by far the most commonly affected, though ingrown nails can occur on any toe. The nail can ingrowing on one side, both sides, or along the full leading edge of the nail.
There are two broad types:
- True ingrown nail — the nail itself is piercing or pressing into the skin at the sulcus
- Involuted (pincer) nail — the nail curves excessively inward, compressing the soft tissue even when the nail edge isn’t visibly breaking through the skin
Both cause pain and both can become infected, but they’re managed slightly differently, which is one reason why self-treatment frequently misses the mark.
What causes an ingrown toenail?
The two most common causes are how the nail is cut and nail shape, but there are several other contributors:
Nail cutting technique Cutting nails too short, rounding the corners, or tearing rather than cutting the nail are the most common causes of ingrown nails we see in practice. When the corner of the nail is cut short or curved, the nail edge can lose its “guide” along the sulcus as it grows out, and the sharp corner drives into the surrounding tissue instead.
Nail shape and genetics Some people simply have nails that are naturally more curved, wider, or involuted. This is partly genetic and means they’re more prone to ingrowns regardless of cutting technique.
Footwear Narrow, tight, or pointed footwear compresses the toes and pushes the soft tissue into the nail edge. Work boots, dress shoes, and tight athletic shoes are common culprits. This is why ingrown toenails are more common in people who spend long hours in enclosed footwear.
Trauma A stubbed toe, dropping something on the foot, or repetitive microtrauma (such as the toe hitting the front of the shoe during running) can cause the nail to grow irregularly.
Excessive sweating (hyperhidrosis) Sweaty feet soften the surrounding skin, making it easier for the nail edge to penetrate.
Nail conditions A fungal nail infection (onychomycosis) thickens and distorts the nail, making ingrowns more likely. Thickened nails are also harder to cut correctly, often leading to techniques that worsen the problem.
Activity and sport Running, football, and other sports that involve repeated forefoot loading, kicking, or sudden stopping are common triggers — particularly in juniors.
What does an ingrown toenail feel like?
The symptoms tend to progress through recognisable stages if left untreated:
Stage 1 — Early
- Pain along one or both sides of the nail when pressed
- Mild redness and swelling at the nail fold
- Discomfort in enclosed footwear or when the toe is touched
Stage 2 — Moderate
- Persistent pain, even at rest
- Increased swelling and redness
- The nail edge is visibly pressing into or under the skin
- Sometimes a small amount of discharge
Stage 3 — Infected / chronic
- Significant swelling, warmth, and redness extending beyond the nail fold
- Pus or discharge at the sulcus
- Overgrowth of granulation tissue (“proud flesh”) — a raised, red, moist lump that bleeds easily
- Pain significant enough to affect walking
- In severe or long-standing cases, infection tracking deeper into the toe
At Stage 3, antibiotics alone will not resolve the problem — the source of irritation (the nail edge) is still there. This is the most common reason people come in having already finished a course of antibiotics and found it made little lasting difference.
Why home remedies don’t fix the underlying problem
We understand why people try to manage this at home first — it feels like it should be simple. But most of the common home approaches either don’t address the cause, or actively make things worse:
Cutting a “V” into the nail This is probably the most widespread ingrown toenail myth. The theory is that cutting a V into the centre of the nail edge causes the sides to “pull in.” In reality, nails don’t grow this way — each part of the nail grows independently from the nail matrix at the back. The V has no effect on the corners at all.
Digging out the corner This sometimes provides brief relief by temporarily removing the offending nail spike — but without proper technique, it usually leaves a sharp spicule behind that continues growing into the sulcus. It also risks introducing bacteria to already-irritated tissue.
Stuffing cotton wool under the nail This can provide temporary cushioning in the very early stages but does nothing to change the direction the nail grows. It’s not a fix; it’s a delay.
Soaking in salt water Warm saline soaks can help with swelling and reduce bacterial load in an early or mildly infected ingrown — and they’re a sensible short-term measure while you’re waiting for an appointment. But they won’t resolve the mechanical cause.
Antibiotics alone Antibiotics treat the infection, not the ingrown nail. Once the course finishes and the nail edge is still there, the infection almost always returns. Recurrent antibiotic use without addressing the nail is a common pattern we see — and it carries its own risks.
The bottom line: if the nail edge is still growing into the tissue, the problem will keep returning until it’s removed.
When should you see a podiatrist?
You should book an appointment if:
- The toe is painful to touch or in footwear and has been for more than a week or two
- There’s visible redness, swelling, or discharge at the nail fold
- You’ve had recurrent ingrown toenails on the same toe
- You’ve finished antibiotics and the toe is still swollen or tender
- You have diabetes, peripheral arterial disease, or compromised immune function — in which case, don’t wait. Foot infections in people with diabetes carry serious risk and warrant early assessment.
- A child has recurring heel or toe pain that’s affecting their sport or sleep
You don’t need a GP referral to see us — you can book directly.
How we treat ingrown toenails
Step 1: Assessment
The first thing we do is have a proper look. We assess the nail’s shape, how far the nail edge has penetrated, whether there’s active infection, whether granulation tissue has formed, and what’s driving the problem in the first place (technique, shape, footwear, fungal changes). This tells us what treatment is appropriate.
Conservative management (early or mild cases)
For very early-stage ingrowns — particularly in children, or where the nail edge is not deeply embedded — it’s sometimes possible to manage conservatively:
- Nail edge debridement: carefully reducing and filing the offending nail edge so it’s no longer pressing into the sulcus
- Taping techniques: using medical tape to gently retract the soft tissue away from the nail edge, giving it room to grow past
- Footwear and cutting technique advice: addressing the cause so the problem doesn’t recur
Conservative management works best in the early stages. For most adults presenting with a recurrent or moderately progressed ingrown nail, it’s not a long-term solution.
Partial Nail Avulsion (PNA)
For recurrent, persistent, or significantly ingrown nails, the definitive treatment is a Partial Nail Avulsion (PNA) — a minor surgical procedure performed in-clinic under local anaesthetic. Here’s what it actually involves:
- Local anaesthetic is injected at the base of the toe. This is the uncomfortable part — brief, sharp, and it’s over within about 30 seconds. After that, the toe is completely numb.
- A narrow strip of nail (the offending edge or edges) is separated from the rest of the nail and removed from the root upwards.
- The nail matrix (the cells at the base of the nail that produce new nail growth) at that edge is treated with phenol — a chemical that permanently destroys that section of the matrix so the problematic edge doesn’t grow back.
- The area is dressed and you’re walking out of the clinic within the hour.
The procedure itself takes about 20–30 minutes. The nail looks almost identical afterwards — just marginally narrower. The vast majority of patients are surprised by how straightforward it is.
Total Nail Avulsion (TNA)
In less common situations — severely deformed or fungal nails, nails that are ingrown along the full width, or nails that have caused repeated problems from both sides — removing the entire nail (with or without permanent matrix destruction) may be the most appropriate option. This is less common and always discussed with the patient beforehand.
What to expect after a PNA
Recovery is generally straightforward:
- The anaesthetic wears off in 2–3 hours. Mild soreness after that is normal; standard analgesics like paracetamol or ibuprofen are usually sufficient.
- The treated area looks worse before it looks better. Some redness, swelling, and discharge over the first few days is normal — this is the body’s response to phenol, not infection.
- Dressings need to be changed daily for the first week to two weeks, depending on healing. We’ll walk you through exactly how to do this.
- Healing is typically complete within 4–8 weeks, though the new nail edge (if not permanently destroyed) takes several months to grow to full length.
- You can walk immediately. Most people return to work the following day, though we recommend closed-in footwear that isn’t too tight for the first week or two.
When phenol is used for permanent matrix destruction, the recurrence rate is very low — under 5% in most published studies.
Will it come back? Preventing recurrence
For patients who’ve had a PNA with phenol, that edge of the nail is gone permanently — it can’t grow back in. So in that sense, the procedure is curative for the treated edge.
For those managed conservatively, or who’ve had the nail edge trimmed rather than removed, recurrence is possible. The best prevention:
Cut nails straight across. The corners of the nail should reach — or slightly extend beyond — the tip of the toe. Don’t round the corners or cut shorter than the end of the toe.
Don’t cut too short. Leave a couple of millimetres of white nail visible at the end. Cutting flush with the skin leaves no guide for the nail to grow over the sulcus.
Choose footwear with adequate toe room. The toe box should allow your toes to sit flat and uncrowded. If your toes are being compressed sideways, the nail has nowhere to go but into the skin.
Treat fungal nail infections. A thickened, distorted nail is much harder to cut correctly and much more prone to ingrowing. If your nails are yellow, thickened, or crumbling, get them assessed.
Keep feet dry. If you sweat heavily, dry feet thoroughly after showering and consider moisture-wicking socks. Softened, macerated skin is much easier for a nail edge to penetrate.
Get regular nail care if cutting is difficult. For elderly patients, people with poor eyesight, or those with limited flexibility who struggle to reach their feet safely, regular podiatry appointments for nail care are far better value than repeated ingrown nail infections.
A note on children and ingrown toenails
Ingrown toenails in children are very common — particularly in active kids playing sport. They tend to respond well to conservative management when caught early, partly because children’s nails are softer and more pliable.
That said, don’t leave a child’s ingrown nail to progress to the infected stage. It’s much more distressing to treat (and for the child to experience) at that point than at Stage 1. If your child is complaining of toe pain, is limping, or you can see redness at the nail fold, bring them in early.
PNA is well tolerated in children and adolescents when conservative care isn’t working. The local anaesthetic is the most significant part, and we’re experienced at making this as comfortable as possible for younger patients.
Ingrown toenail treatment in Newcastle
If you’ve got an ingrown toenail that keeps coming back, isn’t settling, or has become infected — don’t keep putting it off. It’s one of the quickest conditions to fix properly, and genuinely one of the most satisfying for us to treat, because patients walk out of the clinic the same day with the problem solved.
📍 East Coast Podiatry Clinic, 2/1 Glebe St, Kahibah · 📞 (02) 4942 2550 · 🩺 Book online
Frequently asked questions
Does the procedure hurt? The local anaesthetic injection is the worst part — a brief, sharp sting at the base of the toe that lasts about 30 seconds. After that, the toe is completely numb and you feel nothing during the procedure itself. Most patients say it was far less of an ordeal than they expected.
How long does it take? The appointment is typically 30–45 minutes from start to finish, including the consent discussion, anaesthetic, procedure, and dressing. You’ll be walking out within the hour.
Will I need time off work? Most people return to work the next day. We recommend avoiding heavy manual labour or prolonged standing on day one if possible, but there’s no formal recovery period required for most patients.
Is it covered by Medicare or private health? PNA is a minor surgical procedure and may attract a Medicare rebate — we can check your eligibility at the time of booking. Private health extras cover (podiatry) typically applies to the consultation component. Give us a call if you’d like to clarify before booking.
How long until the nail looks normal? If the edge is treated with phenol and won’t regrow, you’ll see a narrow strip of healed skin at the side of the nail. If the matrix is left intact and the nail will regrow (narrower), expect 6–12 months for it to grow to full length.
Can I treat it myself? For a very early-stage ingrown with no infection, a warm saline soak and correctly cutting the nail straight may settle things temporarily. But if it’s recurrent, painful, or infected — come in. Home attempts to dig out the corner almost always make things worse and increase infection risk.
Do I need a referral? No. You can book directly online or by phone.
Medically reviewed by Tim Foran, Podiatrist (AHPRA registered). Last updated: June 2026.